

Post-Exertional Blowback
It's immune. It's metabolic. It's cardiovascular. It is NOT fatigue.

The Science Behind the Payback
Post-exertional malaise (PEM), or post-exertional neuroimmune exhaustion (PENE) is the cardinal feature of ME—and unique to postinfectious disease. Though most of us struggle to find a physician familiar with it, there’s a surprising amount of information out there. PEM, along with the management technique of “pacing,” seems to be the #1 issue raising questions in ME & long Covid groups.
I’m no expert, but I want to gather up some of the information that’s available and put a bunch of it here, in one place, to be reviewed & used in your own time. Particularly when unwell, it can be overwhelming to search for and process information—I hope this post is helpful whether you’re trying to better understand it yourself, or advocate for yourself or a loved one.
Though I usually try to keep posts as short as possible to be “ME friendly,” this one is going to be a bit longer.

PEM = Post-Exertional Malaise
PENE = Post-Exertional Neuroimmune Exhaustion
PESE = Post-Exertional Symptom Exacerbation
It’s a mouthful regardless of which one you prefer to use to describe the primary feature of ME (and, for some, long Covid). Though I believe “PENE” is the best fit for the pathology behind it, I will use the more commonly known “PEM” for the purpose of this post.
PEM is such a weirdo. I don’t think there’s anything else quite like it in terms of its underlying pathology and subsequent symptomatology. As defined above in the OMF graphic, PEM is a worsening of symptoms after exertion. It is not “feeling tired” after exercise. It’s not “feeling tired” at all—which is why I personally think “PEM” doesn’t cover it. ME has been classified as a neurological disease by the WHO; however, the reality is, ME comprises a wider spectrum of physical dysfunction and pathology. ME is immune, endocrine, metabolic, and neurological. Therefore, so are the symptoms and so is PEM.
Myalgic Encephalomyelitis (ME): complex, acquired multi-systemic disease
Pathophysiology: Profound dysfunction/dysregulation of the neurological control system results in faulty communication and interaction between the CNS and major body systems, notably the immune and endocrine systems, dysfunction of cellular energy metabolism and ion transport, and cardiac impairments.
Cardinal symptom: a pathological low threshold of fatigability that is characterized by an inability to produce sufficient energy on demand. There are measurable, objective, adverse responses to normal exertion, resulting in exhaustion, extreme weakness, exacerbation of symptoms, and a prolonged recovery period.
International Consensus Criteria (ICC)—International Consensus Primer
The ICC, quoted above, developed the International Consensus Primer to “utilize current research knowledge to identify objective, measurable and reproducible abnormalities that directly reflect the interactive, regulatory components of the underlying pathophysiology of ME (ME-Pedia).” Basically, to clear some things up.
The diagnostic criteria published by the ICC is a rubric of sorts. The top dog criteria, considered compulsory for diagnosis, is PEM (or PENE as used by the ICC).
Some of the studies the ICC cited regarding PEM include the following conclusions:
abnormal central pain processing during exercise in patients with ME/CFS, both submaximal exercise and self-paced, physiologically limited exercise trigger postexertional malaise in these patients (HERE)
exertion alters gene expression in ME/CFS patients, compared to controls, and some of the genes that were up or down regulated as a result of exertion control pain, fatigue and similar symptoms (HERE)
ME/CFS patients demonstrated significantly lower cardiovascular as well as ventilatory values at peak exercise, compared with the control group; the primary exercise-related physiological difference between the ME/CFS and the control group was their significantly lower heart rate at any equal relative and at maximal work level; assuming maximal effort by all (indicated by measurements and subjective exhaustion), these results could indicate either cardiac or peripheral insufficiency embedded in the pathology of CFS patients (HERE)
PEM is truly all the hazard lights blinking at once. Multiple systems have been studied and shown to be dysregulated. Here’s a nice little 1-minute watch from Long Covid Physio, who state, “Post-exertional symptom exacerbation can be triggered by physical, cognitive, mental, social or emotional exertions, and varies among different people. The worsening of symptoms by exertion can happen immediately, or can happen 24-72 hours after exertion.”
So, PEM is a worsening of symptoms (immediately or delayed) due (in part) to a metabolic deficit triggered by any activity that requires energy—which, is ANYTHING. It takes cellular energy, ATP, to fuel our every movement and thought. When we say “energy” associated with PEM, we’re not talking about good vibes. This is a quantifiable unit of energy that every cell in our body requires to function and we are seeing repeated studies show the underlying pathology includes severe dysfunction in this area. Your level of disease severity typically dictates your level of PEM severity, as well as the level of exertion or effort it takes to trigger it.
Fast forward a few years from the ICC to the 2015 US Institute of Medicine’s (IOM) Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. These criteria for ME/CFS also require PEM for diagnosis. A companion piece was published in the journal Mayo Proceedings titled Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. It explains, “In 2015, the US National Academy of Medicine published new evidence-based clinical diagnostic criteria that have been adopted by the US Centers for Disease Control and Prevention. Furthermore, the United States and other governments as well as major health care organizations have recently withdrawn graded exercise and cognitive-behavioral therapy as the treatment of choice for patients with ME/CFS.” The article was published after input from 21 ME/CFS specialists and aims to make the diagnosis and management of ME accessible to any general practitioner.
In addition to pointing out its delayed onset and prolonged duration, I find this bit refreshing to see highlighted:
Disproportionate intensity. The intensity and duration of PEM are unexpectedly disproportionate to the magnitude of the PEM trigger. For the mildly ill, working a few hours or a day can trigger PEM, whereas for the most severely ill, even basic activities of daily living will be sufficient.
PEM is highly variable across the community and even within individuals. Personally, I experience three kinds of PEM depending on the trigger and my starting baseline: 1) classic flu-like symptoms, 2) full-body pain/discomfort/completely depleted and heavy sensation of all muscles, and 3) cognitive PEM that results in distinct neurological features and cognitive dysfunction.
Some of the studies the IOM cited regarding PEM include the following conclusions:
Changes in brain activity from exertion were significantly related to symptoms for ME/CFS patients. Acute exercise exacerbated symptoms, impaired cognitive performance and affected brain function in ME patients. These converging results, linking symptom exacerbation with brain function, provide objective evidence of the detrimental neurophysiological effects of post-exertion malaise (HERE).
Analysis in 200 ME/CFS patients and 102 healthy individuals showed a specific reduction of amino acids that fuel oxidative metabolism via the TCA cycle; the amino acid pattern suggested functional impairment of pyruvate dehydrogenase (PDH), supported by increased mRNA expression of the inhibitory PDH kinases 1, 2, and 4; sirtuin 4; and PPARδ in peripheral blood mononuclear cells; increased mitochondrial respiration and excessive lactate secretion; findings are in agreement with the clinical disease presentation of ME/CFS, with inadequate ATP generation by oxidative phosphorylation and excessive lactate generation upon exertion (HERE).
The ME/CFS group exhibited significantly reduced anaerobic threshold, heart rate, VO(2) (oxygen your body can absorb), VO(2) peak and peak work compared to controls; when exercising to comparable levels to normal controls, ME/CFS patients exhibit profound abnormality in bioenergetic function and response to it (HERE).
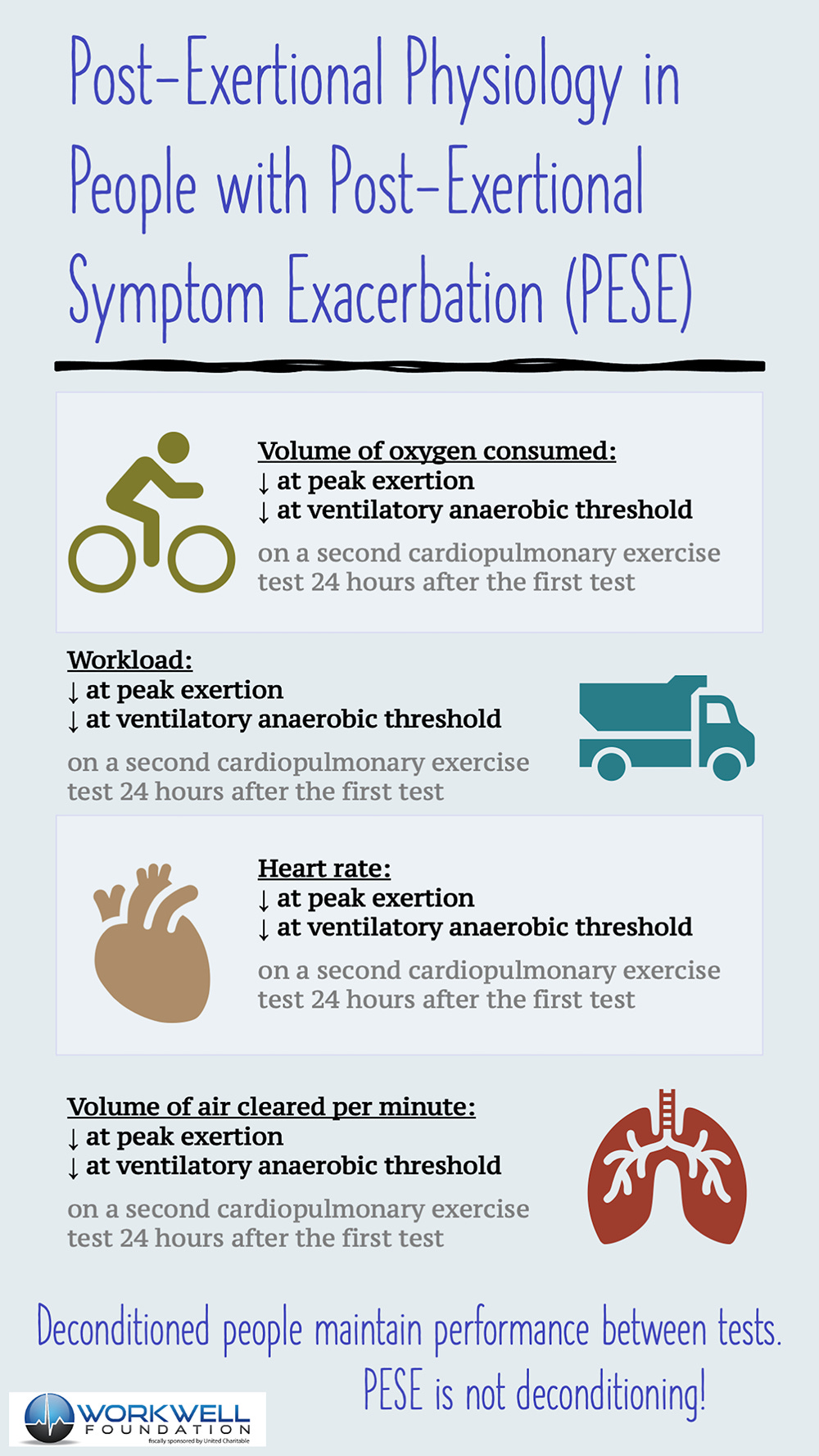
So, now we’re really getting somewhere. Abnormalities in response to exertion is being observed and measured when compared to controls—and studies just keep stacking up. One common way PEM is quantified is through cardiopulmonary exercise testing (CPET) that is designed for ME. The Workwell Foundation has created the gold standard testing procedures to do just that.
Workwell’s mission is to focus on research concerning the functional aspects of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), long COVID, and other fatigue-related illnesses to facilitate an understanding of the biological basis for fatigue and post-exertional malaise (PEM).
We offer 2-day cardiopulmonary exercise testing (CPET) with electroencephalography (EEG) to evaluate functional capacity and cognitive impairment.
CPET is an objective tool that assesses maximal aerobic capacity and sustainable exercise performance, helping identify the origins of aerobic impairment. Aerobic capacity is the maximum amount of oxygen a person can use to produce energy. CPET involves pedaling on a stationary bicycle at a steady pace while the workload, or resistance, gradually increases.
Sampling exhaled breaths during exercise determines oxygen consumption, carbon dioxide production, and pulmonary ventilation. Heart rate, blood pressure, and arterial oxygen saturation are also assessed using a 12-lead electrocardiogram (ECG), blood pressure cuff, and pulse oximeter.
The two-day CPET protocol first researched by Workwell is suited to those with ME/CFS, long COVID, fibromyalgia, and other fatiguing conditions. At Workwell, exercise physiologists and physical therapists with expertise in CPET and fatigue-related illnesses assess post-exertional malaise (PEM) and the ability to work on consecutive days.
This protocol can measure functional impairment during PEM. The first and second tests are separated by 24 hours to allow time to capture symptoms of PEM on the second day. Because a single test does not always show abnormalities, a second test is required, and often reflects how the patient feels when symptoms of PEM flare up.
Here’s a great interview with Todd Davenport PT, DPT, OCS Scientific Advisor to Workwell discussing PEM/PENE (20 min video).
Todd has published a number of studies on PEM, one of which demonstrates clear physiological differences between people with ME and healthy controls (HERE):
“Individuals with ME/CFS and control subjects demonstrated significant differences in CPET measurements at peak exertion during both phases of the 24-hour test-retest CPET paradigm. In this study, all subjects met criteria for peak effort, which allowed for the comparison of physiologically valid CPET data and mitigated the risk for variance due to symptom limited CPET data in a clinical population characterized by disabling fatigue. Compared to control subjects, individuals with ME/CFS demonstrated significantly lower VO2, workload, heart rate, and minute ventilation during Test #1 and Test #2. Effect sizes of between-groups differences were large. These CPET measurements showed further declines during Test #2 in ME/CFS and the significance of between-groups measurements was maintained.”
Check out Todd’s summary of physical abnormalities in people with ME as measured by CPET, HERE.
The Workwell website has a wealth of information, including some very nice educational videos.
I’ve really only scratched the surface, but the studies speak for themselves. It’s outrageous that PEM isn’t universally recognized in medical settings. Unfortunately, it isn’t, and we need to arm ourselves with knowledge before meeting with our doctors. Exercise and physical therapy are recommended to ME patients over and over again in the absence of a PEM screening. This is dangerous. This is foolish. This is a recipe for disease progression.
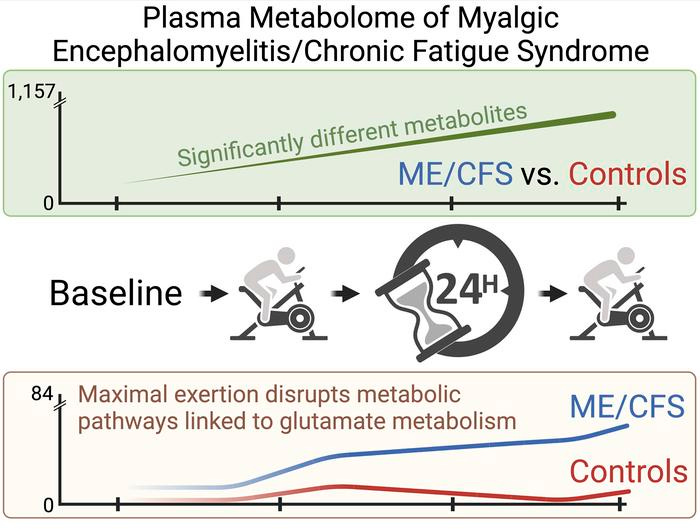
If you’ve hung on this far, I’d like to share just a few more recent studies that have come out of Maureen Hanson’s lab at Cornell, the Center for Enervating NeuroImmune Disease. The first study shows that people with ME show altered metabolic response based on blood samples. The second study shows that women with ME show altered metabolic response based on urine samples. The third study shows a significant difference in recovery time from exertion in patients compared to sedentary controls.
monitored the evolution of 1157 plasma metabolites in 60 ME/CFS and 45 matched healthy control participants before and after 2 maximal CPET challenges separated by 24 hours, with the intent of provoking PEM
The recovery period of participants with ME/CFS is highly disrupted compared with healthy controls.
The effects of exertion in the ME/CFS cohort predominantly highlighted lipid-related as well as energy-related pathways and chemical structure clusters, which were disparately affected by the first and second exercise sessions. The 24-hour recovery period was distinct in the ME/CFS cohort, with over a quarter of the identified pathways statistically different from the controls. The pathways that are uniquely different 24 hours after an exercise challenge provide clues to metabolic disruptions that lead to PEM.
Numerous altered pathways were observed to depend on glutamate metabolism, a crucial component of the homeostasis of many organs in the body, including the brain.
Urine Metabolomics Exposes Anomalous Recovery after Maximal Exertion in Female ME/CFS Patients, 2023
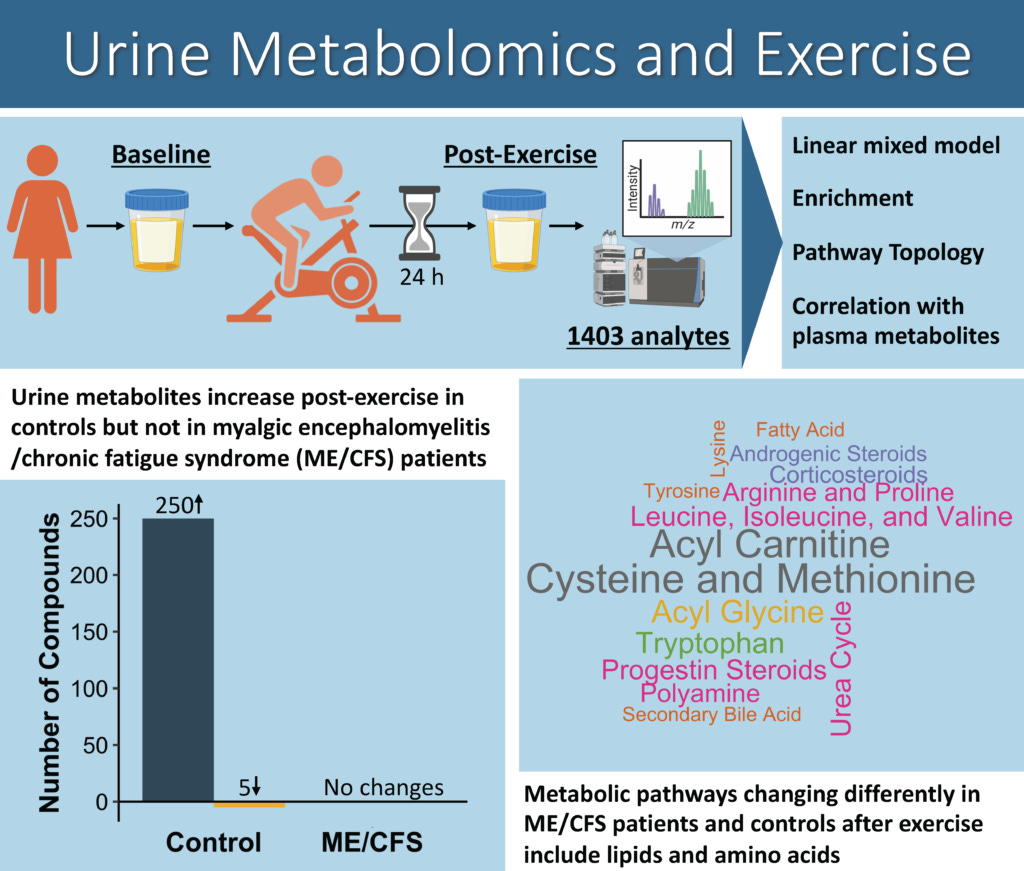
The paper documents a significant difference in recovery between sedentary controls (~2 days) and people with ME/CFS (~13 days).
The range of ME/CFS patient recovery was 1–64 days, while the range in healthy but sedentary controls was 1–10 days; one subject with ME/CFS had not recovered after one year and was not included in the analysis.


I could keep going, but I won’t. If you know or think you have ME/CFS or long Covid with PEM, you will likely deal with doctors who are unfamiliar with it. How can this be with all the studies and all the dedicated researchers finding so many abnormalities?!? Lack of proper funding and medical education has created this absurd situation. One where our cardinal symptom, the thing that can guarantee disease progression, is the thing doctors don’t understand. In fact, we are told to do the exact opposite of the right thing—we are told to exercise and push ourselves. DON’T DO IT.
PEM is horrible to live with. It fundamentally changes every aspect of life. It holds us hostage and puts us in a cage. The more we struggle in that cage, the smaller the cage gets. I will try to publish a future post about “pacing” to discuss the one and only option we truly have.
If you’re living with PEM, be kind to yourself. It is real and it is disabling.
I relate to this post because I think that the term PEM is much like CFS in that it is interpreted by some to mean just the normal tiredness that a person feels after doing something strenuous. But PEM is something that is so hard to explain to others. This article gives a lot of actual measurable examples of what happens to us.
The CPET test is baffling to me. I'm high moderate, borderline severe and have been severe 3 of the past 11 years. I couldn't even get on a bike, never mind thrash out a meaningful result. TWICE!! Since PEM is horrendous, potentially lasts months or longer, and is known to deteriorate....why would anyone try to put a PWME through this? Thank you