
Treatments. Yes, they do exist.
Let's take a deep dive into my treatment regimen.

Thanks to everyone who participated in the reader poll, I’ll be focusing on my treatments in this (long) post. I chose this topic because I encounter people who believe there’s no treatments, no options, & no hope—all the time! Almost daily I encounter someone online who believes this. Don’t get me wrong, there are way too many barriers to treatments and it’s understandable how and why so many people think this. But treatments exist!
Before jumping in I want to acknowledge some of the barriers I mentioned. I want to be clear that receiving treatment is difficult and it’s NOT YOUR FAULT if you’re not receiving treatment. First, finding a doctor willing and able to work with ME patients is a herculean effort. Second, even if your doctor is willing, they still may not be familiar enough with ME treatments to be helpful. Third, money—and more money, is needed to see these doctors and pay for treatment.
Check out this previous post, "Is There a Doctor in the House", to explore resources that help us advocate for ourselves at medical appointments.
The point of this post isn’t to talk exclusively about prescriptions you may not have access to, but I will include them. I’ll cover everything I’m doing that I believe is moving the needle for me.
Big disclaimer: this is not medical advice, everyone’s body and diagnoses behave differently, these treatments may not be recommended for you, and/or may not work for you.
So, onto the daily Ironman of ME treatments!
Pills, Pills, & more Pills: Over the Counter and Prescriptions
If, like me, you’re taking multiple pills several times a day, let me share this gem. This is a handy dispenser that holds a month’s worth of pills with slots four times per day and an alarm. This thing is great! You can find it here: monthly pill organizer with alarm.



Prescriptions
Let’s get these out of the way since you may or may not be able to access them. If nothing else, you can read up on these options and speak to your doctor about them.
Low Dose Naltrexone (LDN): Naltrexone is an opioid receptor blocker traditionally prescribed at much higher doses than what we use for ME. At the very low doses used for ME (and other chronic illnesses), the drug appears to reduce pain, fatigue, and other symptoms (depending on the person). Several studies demonstrate its effectiveness as an anti-inflammatory, pain modulating drug. A 2021 study discusses a potential mechanism by which it’s working for us, essentially “fixing” something broken in our natural killer cells (immune cells that are often found to be dysfunctional in ME).
Low Dose Abilify (LDA): Abilify is another drug being used at a much lower dose than it’s traditionally used. At this lower dose, it behaves very differently and becomes a dopamine system stabilizer. It stimulates the D2 class of dopamine receptors. This 2021 study analyzed the medical records of ME patients using LDA. Of the 101 patients taking it, 74% experienced an improvement in one or more categories: fatigue, brain fog, unrefreshing sleep, and frequency of post-exertional malaise (PEM) episodes, or “crashes.”
Guanfacine: This is an interesting one. Another repurposed drug, guanfacine appears to work on multiple levels. It’s a drug that reduces nerve impulses from the vasomotor center (located in the medulla oblongata of the brain) to the heart and blood vessels. As a result, the heart rate reduces and blood vessels dilate (widen), reducing how hard the heart has to work to pump blood around the body, which lowers blood pressure. So, on this level it can help manage orthostatic intolerance (OI), one of our most common comorbidities. Guanfacine also affects the prefrontal cortex in the brain, which may lend it to reducing other symptoms. A 2024 study demonstrated patients saw improvement in both orthostatic intolerance and fatigue. If, like me, your OI includes periods of low blood pressure, you may need to dial the dose down on this one. As with all these treatments, it’s important to be open to trial and error, have a lot of patience, and maintain consistency.
Tenofovir: Antivirals, where do I even begin?!? I think antiviral use is one of the most complicated topics we face. One of the driving theories behind the pathology of ME is viral persistence—a topic that’s received a lot of attention in light of Long Covid. It makes sense to test that theory with antivirals; unfortunately, our antiviral options aren’t great. In my mind, this is an area we desperately need to improve upon in medicine. My history with antivirals spans multiple doctors including clinical immunologists and ME specialists. I was first placed on Valtrex after an immunologist found my EBV, HHV, and CMV titers were all abnormally high over a prolonged period of time. It seemed to keep some viral-like symptoms in check—until it didn’t. I was then put on Famvir by a ME specialist I previously saw. Same result. Now, under my current specialist, I’m on Tenofovir and have been for about nine months, with a year being the minimum timeframe to be on it. From what I understand, some people respond well to antivirals, but some people don’t respond at all. Sometimes it requires long periods of time before results are seen. Above all, you have to find a prescribing doctor willing to take a chance. For an interesting article that discusses some of the issues surrounding antivirals, go here.
Low Dose Rapamycin: There’s a lot of talk about rapamycin right now in light of Simmaron’s trial, which is on-going. This drug is a mTOR inhibitor and promotes autophagy—autophagy is the cellular process of “cleanup”, when damaged parts of cells are removed and room is made for the generation of healthy cells. There’s evidence that people with ME (or a subset of us) are experiencing a disruption in this process.
According to Simmaron:
Our publication on elevated ATG13 showed that a significant number of ME/CFS patients display serological evidence of autophagy disruption. We have shown that this deficit in autophagy is due to the chronic activation of mTOR. Without properly functioning autophagy, there is significant cellular stress, immune activation, and not enough energy for the cell to do well.
Rapamycin is an mTOR inhibitor. It is an FDA approved drug that was initially developed to protect patients during a kidney transplant. It has a well understood safety profile. This study will track autophagy markers and ME/CFS symptoms in patients who are treated with low-dose rapamycin by participating clinicians.
I’ve now been on rapamycin for 6 weeks. At the low dose, I’m taking it once per week at 1mg, per my doctor’s order. In combination with my other treatments, I believe it’s providing an additional boost. Meaning, more activity tolerance and less PEM. Solve ME will be hosting a webinar in September, if you’re interested in learning more.
Nurtec: Migraines can be common with ME and having a rescue med can be a life saver. Nurtec has worked well for my migraines with aura. Typically, it takes just 30 minutes or so to resolve a migraine once taken.
Singulair: Also called Montelukast, it’s usually prescribed to treat asthma but as a leukotriene receptor antagonist, is also effective for treating mast cell activation. I was originally prescribed singulair for asthma but have found it to be generally helpful since developing ME. Mast cell activation syndrome (MCAS) is another common comorbidity of ME. For more information, here’s a great video.
Over the Counter
It’s easy to talk about accessibility to prescriptions and pretend as if everyone has equal access to over-the-counter treatments—but that’s not true. I’m of the belief that ME requires several (or more) treatment combinations to start moving the needle for moderate to severe people. These OTC options can be really expensive, making them less accessible. I suggest trialing one at a time for no less than two weeks, then stop taking it and observe, then decide if there were worthwhile effects. Last, combine it with the next one and repeat. This can help weed through them, though it’s imperfect. Something may not have noticeable effects on its own but will have effects combined with something else. Trial and error, patience, consistency!
Dextromethorphan: The cough suppressant found in cold medicine? Yes! Dextromethorphan is a NMDA-receptor antagonist and microglial modulator with anti-neuroinflammatory properties. Which means it reduces neuroinflammation, a significant disease process in ME. You can check out my previous post all about it. I take 15mg tablets two to three times per day. I’ve noticed when I stop taking it for a period of time, my cognitive symptoms are worse. My ability to handle more cognitive effort with less PEM is definitely a benefit I’ve noticed.
Ubiquinol: Ubiquinol is the active antioxidant form of CoQ10 and plays a key role in producing cellular energy. It’s a powerful antioxidant that helps protect cells against the damaging effects of oxidative stress, which has been found to be increased in people with ME. I currently take 400mg in the morning.
N-acetylcysteine (NAC): With both anti-inflammatory and antioxidant properties, NAC is often recommended for ME. For a deeper dive into the specifics, check out this article. I’m currently taking 1,000mg per day but have taken twice that amount in the past. There’s been a small study evaluating the effects of combining NAC with guanfacine (discussed above). They found some improvement was made by reducing cognitive symptoms. As someone who happens to take both of these, I would agree with that.
Alpha-lipoic acid (ALA): Another antioxidant! ALA is a fatty acid that helps convert glucose to energy via aerobic respiration. And as we all know, we need all the help we can get with that! I take between 250 - 500mg per day.
H1 and H2 Blockers: Common antihistamines like pepcid and zyrtec are designed for allergy symptoms but can provide a broader spectrum of relief in ME and Long COVID. Histamine is a chemical the immune system releases to send messages between different cells and these blockers help reduce that activity. It appears in ME and Long COVID, the benefits of antihistamines go beyond allergy symptoms. The American ME/CFS Society has an interesting compilation of studies here.
Curcumin: Curcumin is the main active ingredient in turmeric and has powerful anti-inflammatory and antioxidant properties. I take 1,000mg daily. Here’s a 2018 study claiming positive outcomes after an 8-week trial for people with ME.
Vagus Nerve Stimulation
“Vagus nerve stimulation involves using a device to send electrical impulses to the vagus nerve. The vagus nerve is the main nerve of the system that controls digestion, heart rate and other vital functions. When the device fires, it sends electrical impulses to areas of the brain. This changes brain activity to treat certain conditions,” Mayo Clinic.
I’m a big fan of this treatment but it takes time and consistency to start seeing results. Vagus nerve stimulation (VNS) significantly improves my GI symptoms, reduces my cognitive dysfunction, and contributes to less PEM. I would say it took a solid 3 months before I started noticing anything, 6 months before I started noticing moderate improvement, and a year before it really started to work its magic. Now, if I accidently miss a few days, I start having GI symptoms until I start up again. I consider VNS to be a critical part of my treatment protocol.
The devices most often used are “transcutaneous,” or used against the skin to transmit the electrical impulses. I use the Truvaga device, which is held up against the left side of the neck. I chose this device because it’s made by the same company that makes one of the few FDA approved transcutaneous VNS devices (which requires a prescription). This gave me more confidence that Truvaga is “dialed in” for safe and effective VNS. Not to say others aren’t, this was just my personal comfort level.

The vagus nerve is the longest and most complex cranial nerve in your body, wandering and branching from the brain to your abdomen. One of its major functions is to balance the nervous system between the sympathetic side and the parasympathetic side. It regulates our “fight or flight” and “rest and digest” responses from these two sides of the nervous system. Here’s an interesting 2020 study that examined VNS in people with “moderate to severe ME.” The study found significant symptom relief in the treated individuals compared to the placebo group. If you’re on Facebook, there’s a great group for VNS guidance called “AVA A Vagus Adventure”.
The following video advertises the newer version of the device. Please be aware this video plays music and is visually stimulating.
Pacing with Visible
Pacing may seem more “lifestyle” than “treatment”, but I would argue that pacing with a tool designed for chronic illness is 100% treatment. I’ve found the Visible heart rate monitor and app to be life changing. Use this link to get $20 off!

Admittedly, it took me a solid year of use before genuinely understanding how to take the information from this tool and apply it to my life via pacing. While working with an occupational therapist trained in ME (Amy Mooney), I was able to slowly grasp the true breadth and depth of pacing. That’s when the power of Visible became clear.
The app connects to a continuous heart rate monitor you wear. You earn points based on your heart rate and those points are a measure of your pacing. After a few weeks of use, you can begin to determine how many points are too much—invoking PEM or crashes—and how many points are safe to use in a day. Then, you set your daily point budget and try to stay below that number. The app also tracks symptoms you log and gives you an opportunity to look at and compare trends. One of its most unique features is the morning check-in, which provides a daily score based on baseline. It measures your resting heart rate and heart rate variability and compares it to a running average. My morning check-in can tell me when I need to pace more carefully for that day and it’s usually right!
The number of points required to do normal activities of daily living will probably blow your mind! You’ll quickly find out exactly why it’s so difficult for us to shower, cook meals or do laundry, for example. Quantifying the otherwise nebulous world of pacing is a game changer. Using Visible has been critical for me, but it takes some time to navigate. If you try it and need some help figuring it out, drop me a line.
Use this link to get $20 off!
Here’s an interview with the co-founder of Visible:
Metabolism Tracker: Lumen
Ok, at this point it’s becoming pretty obvious that I’m a bit of a gadget nerd. It’s true. But I’m a huge proponent of biometric feedback and using it to leverage any and all advantage we can find. Lumen is a device you breathe into, and it tells you the ratio of carbs to fat that you’re burning at that moment—anaerobic vs. aerobic respiration. I consider this device part of “treatment” because it’s helping me make lifestyle changes that I believe are relevant to symptom management.
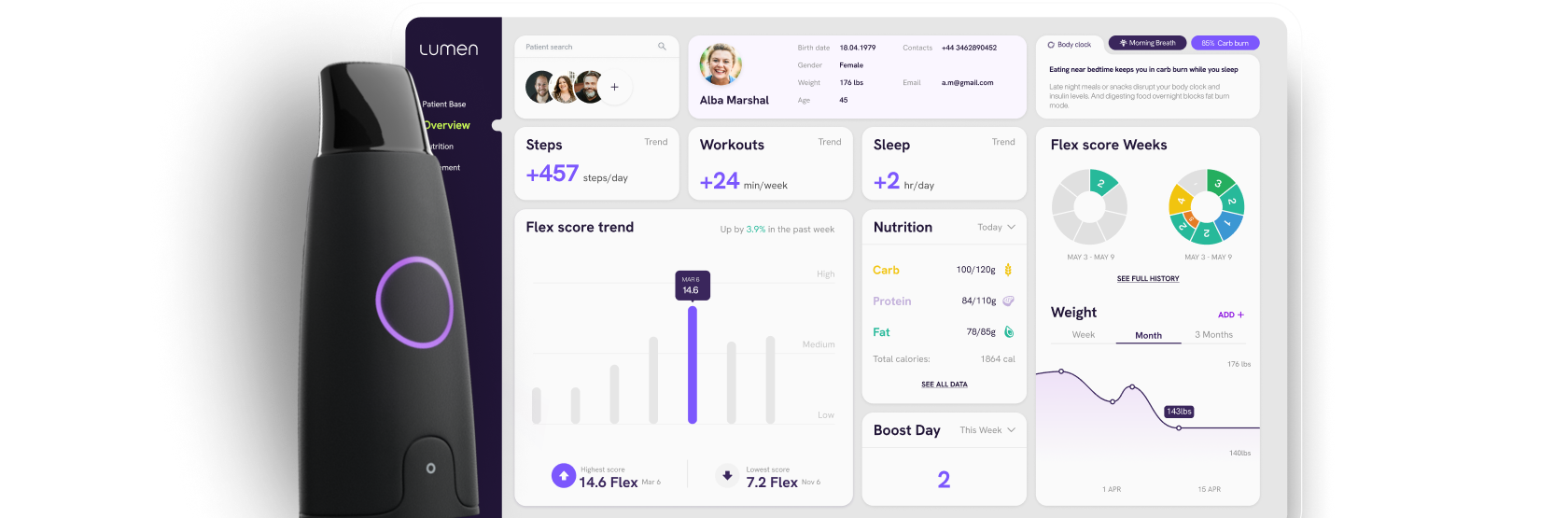
This device is not designed for medical issues or chronic illness. It’s designed to help people maximize their metabolic flexibility for purposes of weight loss/gain, feeling better in general/energy, athletic performance, etc. However, when I read about its capabilities, I immediately thought ME. It’s well known that people with ME have a lower anaerobic threshold. We switch from aerobic to anaerobic metabolism much easier than healthy people and this means we’re not capable of producing the proper amount of cellular energy for activities. Having a device to tell us when (and maybe why) we’re switching would be amazing—and I think that’s what this device does.
For instance, I’ve learned from this device that being in a carb deficit in my diet pushes me to burn carbs (anaerobic). Whereas if I eat the right amount of carbs during the day I tend to stay in fat burn (aerobic) more often and for longer periods of time. This is helpful since burning fat is a more energy efficient metabolic state. I’ve also learned that finishing my food for the day about 3 hours before bed and extending my overnight fast later into the morning/early afternoon keeps me in fat burn. And with the Lumen I can see exactly when my body starts to switch to carb burn post fast, which tells me to eat.
Given the problems we have with energetics, I think it’s important to take your time with this device. Get to know its capabilities and what your data means before rushing into lifestyle changes. Just my 2 cents!
Use this referral code to get $40 off: NREF_dsD43
Other
A few more things. Hydrate, hydrate, hydrate. Orthostatic intolerance is so common with ME. I have POTS but you may not have an official diagnosis. Without one, here’s a simple thing you could do to test out its impact. Hydrate well for a few days and include electrolytes. If you notice any improvement at all, you may be on to something. This is one of my preferred electrolytes, though there are many on the market now.
Occasional additions to my regimen include red light therapy and leg compression. I’m not convinced these things contribute greatly to reduced symptoms, but I do use them. You can read more about red light therapy here. Leg compression can help with circulation, and this might be of greatest benefit for orthostatic issues. There are lots of options for this, including these.
Conclusion
Well, there it is. I honestly don’t think there’s one silver bullet for treating complex multi-system diseases. The complexity involved seems to necessitate, at least for now, the right combination that fits the individual. The treatment regimens for people with ME or Long COVID may seem like “overkill”, but I believe efficacy is coming from the combinations and not necessarily any one thing in particular.
Based on my experience, I think the three most important things with treatments is being systematic, patient, and consistent. And remember, not everyone responds to the same treatments the same. If you don’t respond to something, it’s ok to move on to something else.
I realize accessibility is a real issue for our community and that includes affordability. If you’re struggling to work here in the US and think disability may be your next stop, here’s a previous post to walk you through the process.
I wish I could bundle up the success I’ve had with treatments and hand it out to everyone struggling. I hope this information is at least a little helpful. You can also follow me on Instagram where I’ll try to upload some videos of the devices I’ve discussed above, @mkaysen417.
Take care, as best you can.
I would add as a component of pacing, mobility aids have been huge! I have a cane, walker, and wheelchair. I use them liberally and without shame. Don’t ever hesitate to use them if they make sense for you.
Treatment regimen buddies! I’m on the same meds, plus a few more (mostly mast cell stabilizers). Love and solidarity to you. Thanks for publishing this vital information; I think I’m going to do the same at some point soon.